Content
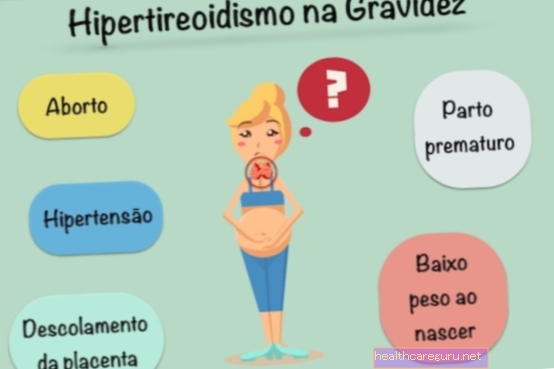
Hyperthyroidism can appear before or during pregnancy, and when left untreated it can cause problems such as premature birth, hypertension, placental detachment and abortion.
This disease can be detected through a blood test, and its treatment is done with the use of drugs that regulate the functioning of the thyroid. After delivery, it is necessary to continue medical monitoring, as it is common for the disease to remain throughout the woman's life.
Symptoms of hyperthyroidism in pregnancy
The symptoms of hyperthyroidism in pregnancy can often be confused with symptoms that arise due to the hormonal changes common in pregnancy, and there may be:
- Excessive heat and sweat;
- Tiredness;
- Anxiety;
- Accelerated heart;
- Nausea and vomiting of great intensity;
- Weight loss or inability to gain weight, even if you eat well.
Thus, the main sign that something may be wrong with the thyroid is the lack of weight gain, even with increased appetite and the amount of food consumed.
It is important that the woman is regularly monitored by the doctor so that tests can be performed to help assess the general health of the woman and the baby. Thus, in this case, T3, T4 and TSH blood dosage can be recommended, which when in increased amounts may be indicative of hyperthyroidism.
However, it is important to remember that the hormone T4 may be elevated due to high levels of beta-HCG in the blood, especially between the 8th and 14th week of pregnancy, returning to normal after this period.
How to treat
The treatment of hyperthyroidism in pregnancy is done with the use of medications that help to regulate the production of hormones by the thyroid, such as Metimazol and Propilracil, which should be used according to the doctor's guidance.
At the beginning, larger doses are given to control hormones more quickly, and after 6 to 8 weeks of treatment, if the woman improves, the dose of the drug is reduced, and may even be suspended after 32 or 34 weeks of gestation.
It is important that treatment is carried out according to medical advice, because otherwise high levels of thyroid hormones can lead to the development of complications for both mother and baby.
Possible complications
The complications of hyperthyroidism in pregnancy are related to the lack of treatment or incomplete treatment for hyperthyroidism, which can result in:
- Premature birth;
- Low weight at birth;
- Hypertension in the mother;
- Thyroid problems for the baby;
- Placental displacement;
- Heart failure in the mother;
- Abortion;
It is important to remember that in most cases, women already had symptoms of the disease before pregnancy and therefore do not notice the changes caused in the body when they become pregnant. The main cause of hyperthyroidism is Graves' disease, which is an autoimmune disease in which the cells of the immune system attack the thyroid gland itself, resulting in deregulation of hormone production. See more about Graves' disease.
Postpartum care
After delivery, it is necessary to continue taking the drugs to control the thyroid, but if the medication is discontinued, new blood tests should be done to evaluate the hormones 6 weeks after delivery, as it is common for the problem to reappear.
In addition, during the breastfeeding period it is recommended that medications be taken in the lowest possible doses, preferably right after the baby is breastfed and according to medical advice.
It is also important to remember that children should have routine tests to assess thyroid function, as they are more likely to have hyper or hypothyroidism.
See feeding tips to treat and prevent thyroid problems by watching the following video: